- Last edited on September 5, 2023
The Neurological Exam
Primer
The Neurological Exam is an important physical examination for not just neurologists, but also psychiatrists. This is particularly important to rule out neurological causes of psychiatric disorders, and in even more so in older adults, where neurodegenerative disorders are more prevalent.
See NeuroExam.com for videos of specific exams
You can refer to NeuroExam.com for a demonstration of each neurological exam. Each section below will also link to other neurological exam videos as well.Appearance and Mental Status
- Handedness (left/right/ambidextrous)
- Orientation (person, place, time)
- Observe for:
- Titubation, involuntary tremor that occurs in the head, neck, and trunk area (this is an essential tremor, which causes uncontrollable, rhythmic shaking)
Language
Language can also be assessed using common cognitive tests. A focus should be on:
- Fluency
- Paraphasias
- Anomia
Primitive Reflexes
Even healthy individuals can have 1-2 primitive reflexes present (also known as frontal release signs), but if more are present, this suggests a neurodegenerative disorder.
Frontal Release Signs
| Test | Exam | Pathological Response |
|---|---|---|
| Glabellar tap | Tap patient's forehead repeatedly | Normal patients will blink in response to the first several taps. However, if the blinking persists, this is known as Myerson's sign, and is often seen in Parkinson's. |
| Palmnomental | Use your nail to strike then thenar eminence briskly (you want to give a noxious stimuli) | The ipsilateral mentalis muscle of the lower lip contracts. It is a low sensitivity, high specificity sign.[2] |
| Grasp reflex | Grasp patient's hand and rub your hands along the palmar surface | Patient's hand will grasp your hand (watch out, this can sometimes be really strong!) |
| Pout reflex | A tongue depressor is pressed on the lips | Pouting of the lips |
| Rooting reflex | Gently stroke the lateral upper lip | The mouth to moves toward the stimuli |
Cognitive Assessment
Cognitive testing is again relevant in older adults and middle age adults that present with psychiatric symptoms. Some neurodegenerative disorders may present initially with a prodrome of anxiety or depression even prior to the development cognitive symptoms.
Other things to assess for include:
Cranial Nerves (CN)
Full Cranial Nerve Exam Video
CN I
Cranial Nerve I
Olfactory (1) nerve| Test | Exam | Normal finding | Pathological finding | Disease/Lesion | Video |
|---|---|---|---|---|---|
| Smell | Ask patient to identify odours (e.g., mint, soap, coffee) to each nostril while the other nostril is occluded | Patient is able to smell | Anosmia (unable to smell) | Parkinson's, fronto-orbital head trauma, sinus infection | - |
CN II
Eye Exam Videos
Cranial Nerve II
Optic (2) nerve| Test | Exam | Normal finding | Pathological Finding | Disease/Lesion | Video |
|---|---|---|---|---|---|
| Pupil size | Observe the size of the pupils | 2-4mm in bright light 4-8mm in dim light | Unequal pupil size, or diameter beyond normal findings | Can be physiological, pathological or pharmacological | - |
| Fundoscopy | Use a fundoscope to examine the back of the eye | Macula can be visualized. Sharp optic discs with no vascular changes. Venous pulsations are present bilaterally. | Engorgement of retinal veins, deep haemorrhages, cotton wool spots and/or optic disc swelling | Macular or vascular disease | - |
| Pupillary light reflex | Shine a light directly into the eye and observe for constriction | Pupil constricts when light flashes on same side | Fixed pupils or sluggish constriction | Lesion or disease along retina, optic nerve, and/or brain | - |
| Swinging light test | Light is alternately shone into the left and right eyes (“swinging”) | Equal constriction of both pupils at the same time, regardless of which eye the light is directed at (indicates an intact direct and consensual pupillary light reflex) | Relative Afferent Pupillary Defect (RAPD) or also known as Marcus-Gunn pupil. • Light shone in the affected eye → cause only mild constriction of both pupils (due to decreased response to light from the afferent defect). • Light shone in the unaffected eye → cause normal constriction of both pupils | Lesion of optic nerve, visual pathway, retina, or amblyopia | • Relative Afferent Pupillary Defect (RAPD) Example • Relative Afferent Pupillary Defect (RAPD) and Marcus-Gunn pupil |
| Visual fields (central and peripheral) | Position yourself at arm's length away from the patient. Your eye should be open to the same side as your patient's open eye (this will align your visual fields). Ask how many fingers are seen in each of the quadrants. | Visual fields are full to confrontation (or full to finger counting) | Visual field defect (e.g. - hemianopia). For example, in homonymous hemi-anopsia, this is the losing of one half of their side vision on the same side in both eyes. “Homonymous” refers to having the same, “Hemi” refers to half and “Anopsia” refers to blindness. | Optic nerve or visual cortex lesions | • Visual Field Testing • Visual Field Defects |
| Visual acuity | Use a Snellen chart, and test each eye individually | 20/20 vision in both eyes | Any change in visual acuity | Optic nerve or visual cortex lesions | - |
CN III, IV, VI
Cranial Nerve III, IV, VI
Oculomotor (3), trochlear (4), abducens (6) nerve| Test | Exam | Normal finding | Pathological finding | Disease/Lesion | Video |
|---|---|---|---|---|---|
| Extra-ocular eye movements (EOMs) | Look at the patient's eye movements as they follow yours finger's movement in the H-shape | Eyes are able to track the H-shape fully | Limits in patient's gaze or ability to look in certain directions, such as an Internuclear Ophthalmoplegia (INO) | • Restricted vertical saccades and vertical gaze palsy is suggestive of PSP • INO can be indicative of diffuse MS, stroke, or brain stem lesion | • INO • Vertical Gaze Palsy in PSP • Horizontal and vertical gaze centers |
| Smooth pursuit during EOM | Look at the patient's eye movements as they follow yours finger's movement in the H-shape | Smooth pursuit with no nystagmus (no beating movements) | Nystagmus | Smooth pursuit can be impaired in Parkinson's [3] | • Smooth pursuit • Nystagmus |
| Saccades | • Reflexive: Ask patient to quickly change focus from one fixed point to another repeatedly (e.g. - finger-pen-finger) • Volitional: Ask patient to look up to the ceiling and down to the ground without shifting head position | Fast and accurate saccades (however, saccades do slow down with age[4]) | Saccadic intrusions such as square wave jerks (SWJ), square wave pulses (SWP), macrosaccadic oscillations, saccadic pulses, ocular flutter, and opsoclonus. | Restricted vertical saccades and vertical gaze palsy is suggestive of PSP. | • Saccades • Saccades • Impaired saccades |
| Oculocephalic (“Dolls Eyes”) maneuver | Ask patient to keep eyes locked and fixed onto your face, and move head up, down, left, and right. | Patient will maintain forward gaze as their head is turned | Lesion in the labyrinth or vestibular lesion | If there is impaired gaze, but VOR is normal, then suggestive of PSP | Oculocephalic reflex and its role in PSP diagnosis |
CN V
Cranial Nerve V
Trigeminal (5) Nerve| Test | Exam | Normal finding | Pathological finding | Disease/Lesion | Video |
|---|---|---|---|---|---|
| Sensory (Facial Sensation) | Use cotton swab (or pin) to touch in V1, V2, and V3 distribution of the nerve | Same sensation on both sides | Altered sensation on one side | Trigeminal nerve lesion | - |
| Motor (Muscles of mastication) | Observe muscle bulk and atrophy, ask patient to clench jaw and feel for muscles | Good strength bilaterally, feeling of muscle contraction, and no atrophy | Muscle weakness | Trigeminal nerve lesion | - |
| Corneal reflex | Out of the corner of patient's eye, use the tip of a tissue paper and lightly brush on the cornea | Reflexive eye blink to the noxious stimuli | Absence of reflexive eye blink | Trigeminal nerve lesion | - |
| Jaw jerk reflex | Open the mouth and and gently strike the jaw with a reflex hammer, | Looking for exaggerated response |
CN VII
Cranial Nerve VII
Facial (7) Nerve| Test | Exam | Normal finding | Pathological finding | Disease/Lesion | Video |
|---|---|---|---|---|---|
| Inspection | Look for facial (eyes, lips) drooping or facial asymmetry | No facial drooping | Facial drooping or weakness | Lesion to facial nerve or stroke | - |
| Muscles of facial expression | • Scrunch forehead (wrinkles) • Close eyes tightly (“don't let me open them”) • Show teeth and nice big smile • Puff out cheeks | Good strength bilaterally to muscles of facial expression | Facial drooping or weakness | Lesion to facial nerve or stroke | - |
CN VIII
Cranial Nerve VIII
Vestibulocochlear (8) nerve| Test | Exam | Normal finding | Pathological finding | Disease/Lesion | Video |
|---|---|---|---|---|---|
| Cochlear branch of nerve | • Hearing using gentle whispering in each ear • Weber and Rinne Test | Able to hear whisper on each side | Unable to hear | Weber and Rinne | |
| Vestibular branch of nerve | Head Impulse Nystagmus Test of Skew (HINTS) | See video | See video | HINTS Exam | |
| Dizziness | Dix-Hallpike Maneuver | See video | See video | Dix-Hallpike Test & Epley Manoeuvre |
CN IX and X
Cranial Nerve IX and X
Glossopharyngeal (9) and Vagus (10)| Test | Exam | Normal finding | Pathological finding | Disease/Lesion | Video |
|---|---|---|---|---|---|
| Inspection | Tell patient to say “Ahh” | Palate and uvula midline | Deviation of palate and midline | - | |
| Gag reflex | Put tongue in the back of the throat | Gag reflex | - | - | |
| Phonation | Listen to patient's voice during exam, ask patient to repeat sounds: “Ka, Ka, Ka” “Ma, Ma, Ma” “La, La, La” | Normal phonation and voice | Hoarse voice | Lesions (e.g. - mediastinal lymphoma, aortic aneurysm) compressing the recurrent laryngeal nerve | - |
CN XI
Cranial Nerve XI
Accessory (11) nerve| Test | Exam | Normal finding | Pathological finding | Disease/Lesion | Video |
|---|---|---|---|---|---|
| Sternocleidomastoid | Look at sternocleidomastoid, palpate, and tell patient “push against my hand with your neck” | Head turning strength is intact and equal on both sides | Weakness on one or both sides | Lesion of accessory nerve | - |
| Trapezius | “Shrug your shoulders up against my hand” | Shoulder shrug strength equal on both sides | Weakness on one or both sides | Lesion of accessory nerve | - |
CN XII
Cranial Nerve XII
Hypoglossal (12) nerve| Test | Exam | Normal finding | Pathological finding | Disease/Lesion | Video |
|---|---|---|---|---|---|
| Tongue atrophy | Ask the patient to extend the tongue and inspecting it for atrophy | No fasciculations, no atrophy, no weakness or deviation of tongue | Fasculations, atrophy, weakness/deviation | Lesion of hypoglossal nerve | - |
Motor
- Muscle (primarily examine the four limbs)
- There should be full range of motion of joints with full resistance to opposition in upper and lower extremities
- Bulk
- Examine the thenar eminence muscles, and look for flattening or atrophy (an early sign of ALS)
- Strength
- There should be good strength against opposition in all limbs
- Tone
- There should be firm muscle tone, without spasticity, atrophy, or abnormal movements in the upper and lower extremities.
Upper Motor Neuron Lesion Tests
| Test | Exam | Pathological Response | Video |
|---|---|---|---|
| Pronator drift | Patient seated, arms flexed at shoulders at 90 degrees, elbows fully extended, and hands supinated. Then instruct patient to close eyes for 15-30 seconds. | A normal test is the patient should be able to maintain this position for the duration of closing their eyes. In a positive test, the one hand may drift down and away (i.e. - pronation) | Pronator drift |
| Forearm rolling (“Satellite sign”) | Patient flexes elbows at 90 degrees, and places forearms parallel to each other in front of the torso, and rotates forearms in front of eah other for 5-10 seconds. | The affected arm will remain stationary, while the unaffected side will revolve around it like a “satellite.” Cortical lesions affect the contralateral arm. Cerebellar lesions affect the ipsilateral arm.[5] | - |
| Forearm/thumb rolling | Same as above but with thumb or fingers | Same as above but with thumb or fingers | - |
Comparison of Upper Motor Neuron vs. Lower Motor Neuron Lesions
| Sign | UMN Lesion | LMN Lesion |
|---|---|---|
| Weakness | + | + |
| Atrophy | - | + |
| Fasciculations | - | + |
| Reflexes | ↑ | ↓ |
| Tone | ↑ | ↓ |
| Babinski | + | - |
| Spastic paresis | + | - |
| Flaccid paralysis | - | + |
| Clasp knife spasticity | + | - |
Mnemonic
- Lower motor neuron = everything lowered (less muscle mass,muscle tone,reflexes, downgoing toes)
- Upper motor neuron = everything up (tone, DTRs, toes)
- Fasciculations = muscle twitching
- Positive Babinski is normal in infants
Hypertonia (Rigidity, Spasticity, and Paratonia)
Hypertonia (i.e. - resistance to movement) can be due to one of 3 causes:[6]
- Spasticity (results from increased deep tendon reflexes due to hyperexcitability of the muscle's stretch reflex)
- Rigidity (suggests basal ganglia dysfunction on the contralateral side. The most common cause is Parkinson's disease)
- Paratonia (inability to relax muscles during muscle tone assessment, can be seen in dementia and catatonia)
- Gegenhalten (German for “against-stop”, or oppositional paratonia), which is an inability for the patient to relax the limb fully for the examiner to perform testing of passive range of motion
- Mitgehen (facilitatory paratonia), in which the patient tries to help out the examiner as the examiner tries to passively move the limb, despite instructions to remain still. This is in contrast to Gegenhalten, where the patient resists against the movements of the examiner.
Hypertonia Videos
Hypertonia
| Spasticity | Rigidity | Paratonia | |
|---|---|---|---|
| Causes | • Stroke, cerebral palsy, multiple sclerosis • Spinal cord disease/compression • Upper motor neuron disease | • Extrapyramidal lesions (e.g. - in Parkinson's) • Extrapyramidal side effects (EPS), most commonly from antipsychotics | • Dementia • Catatonia |
| Neuroanatomical Location | Corticoreticulospinal (pyramidal) tracts | Extrapyramidal pathways (most commonly basal ganglia) | Bilateral frontal lobe dysfunction (non-specific) |
| Exremity Weakness | Yes | No | No |
| Resistance | More resistance in one direction than the other direction | Same resistance throughout | Variable |
| Tone | Greater tone in initial part of movement (i.e. - “clasp knife spasticity”) | Same tone throughout (described as the feeling of a metal being bent, i.e. - lead pipe rigidity) | • Gegenhalten (oppositional paratonia) occurs when subjects involuntarily resist to passive movements • Mitgehen (facilitatory paratonia) occurs when subjects involuntary assist passive movements |
| Velocity Dependent | Yes (i.e. - the faster you go, the more resistance you feel) | No (does not vary with speed of movement) | Yes (oppositional paratonia increases with movement velocity)[7] |
| Other Exam Findings | • Upgoing Babinski reflex • Characteristic pattern: prominent in the flexors of the upper extremity and the extensors of the lower extremity. | • Rigidity can be brought out or aggravated by the activating the contralateral limb (e.g. - by asking patient to open and close their contralateral hand) This is a phenomenon known as activated rigidity.[8] | • Other features of catatonia may be found |
Tremors
- Postural/action tremors = tremor throughout movement
- Intention tremor = more like ataxia, they have side-to-side tracking at the end and over shooting
- Resting tremors
- Psychogenic tremors[9]
Myoclonus and Clonus
Myoclonus (myoclonic jerks) refers to sudden, (i.e. - quick) brief involuntary twitching or jerking of a muscle or group of muscles. A variety of metabolic disturbances, such as hyperammonemia, electrolyte derangements, uremia, and hypercarbia can all cause myoclonus. Importantly, medications such as opioids and gabapentin can also cause myoclonus (especially in the setting of acute kidney injuries when gabapentin is not able to be cleared).[10]
- Positive myoclonus is due to a jerky contraction of a muscle. Everyone has positive myoclonus sometimes (hiccups!)
- Negative myoclonus (also known as asterixis) is due to a pathological relaxation of a muscle.
- Why is asterixis examined in the “stopping traffic” position with the patient's hands? It requires constant activation of wrist extensors, so when there is pathological relaxation, the hands drop and recover.
Myoclonus Examination
| Test | Exam | Pathological Response |
|---|---|---|
| Asterixis | The patient extends their arms, dorsiflex their wrists, and spreads their fingers (similar to pushing against a wall or “stopping traffic”) with their eyes closed. | The presence of “flapping” hands indicates the presence of asterixis, which is a non-specific sign for hepatic encephalopathy. |
Clonus, on the otherhand, is rhythmic or regular, and related to lesions in upper motor neurons (e.g. - stroke) and is generally accompanied by hyperreflexia. Syndromes such as serotonin syndrome can also result in clonus.
Clonus Examination
| Test | Exam | Pathological Response |
|---|---|---|
| Clonus | Examiner dorsiflexes the patient's foot (so their toes are pointing upward), and then holds the foot there. | Normal patients may have one or two beats. A series of beats may indicate clonus. Clonus is a marker of hyperreflexia, which is part of an upper motor neuron syndrome. |
Cogwheeling
Cogwheel rigidity, a feature of Parkinson's, is really just a combination of rigidity plus tremor. The “cogwheeling” is always the same frequency as the tremor.
Coordination
- Dysmeteria
- Finger-to-nose testing
- Heel-to-shin
- Dysdiadochokinesia
- Test rapid alternating movements (RAM)
- Finger tapping and toe tapping (is there diminished movement suggestive of Parkinson's Disease?)
Gait Exam Videos
Tests of Coordination
| Test | Exam | Pathological Response |
|---|---|---|
| Rapid alternating movements (RAM) | Ask patient to rest one hand and another, then alternate quickly one hand between supination and pronation. | When a patient has cerebellar disease, one movement cannot be quickly followed by its opposite and movements are slow, irregular, and clumsy. This condition is called dysdiadochokinesis. |
| Finger-to-nose testing (FNT) | Ask the patient to touch your finger, then touch their nose. Their arms should be close to fully extended. Repeat this task several times. | In a patient with cerebellar disease, movements of the ipsilateral extremity are clumsy, unsteady. It will also varying in speed, force, and direction. This is called dysmetria. FNT also tests for something separate and unrelated: action tremors. This is unrelated to dysmetria. The difference between tremor and dysmetria is that tremors are rhythmic and oscillatory, whereas dysmetria is more unpredictable and usually results in an overshoot or undershoot of a target. |
Gait
- Both gait ataxia and gait apraxia are commonly associated with subjective balance difficulty and falls. However, they present different clinically and have different lesion localizations.
- Gait ataxia has a wide-based gait and difficulty standing with the feet together. Ataxia can be checked for if the Romberg sign is present (i.e. - the patient can stand with feet together and eyes open but cannot balance if their eyes are closed or in the dark).
- In severe gait or postural ataxia, patients cannot even stand with their feet together even with eyes open.
- Gait ataxia is due to incoordination of the lower extremities due to central cerebellar pathology (also called cerebellar ataxia) or loss of peripheral proprioceptive input (also called sensory ataxia).
- Cerebellar ataxia can be due to vascular, toxic (e.g. - alcohol), degenerative (e.g. - hereditary cerebellar ataxias), inflammatory (e.g. - multiple sclerosis) or neoplastic causes.
- To differentiate between cerebellar ataxia vs. sensory ataxia, an individual's Romberg test will improve (i.e. - they become more stable) if their eyes are open (i.e. - the loss of proprioception may partially be compensated by visual input by open their eyes).
- Gait apraxia on the other hand, involves having a hard time getting started with walking and may look like a “magnetic” or shuffling gait.
- Individuals will typically have an erect posture, slightly broad-based stance, difficulty initiating gait, reduced cadence (steps per minute), and short shuffling/hesitating steps, as if their feet were “glued” to the floor
- Gait apraxia can be seen in dementia (in particular with vascular dementia) and in normal pressure hydrocephalus.
- Since gait apraxia is a motor planning deficit, it thus has a cerebral (not cerebellar, and not peripheral) lesion localization.
- In gait apraxia, remember that the abnormality is restricted to walking only and there is no motor weakness in the lower limbs, no sensory loss in the lower limbs, and no cerebellar dysfunction to account for the gait difficulty.
Gait Exam
- When doing a walking gait exam, assess for the following:
- Gait base: is there a wide base, narrow base, or normal base of support?
- Arm swing: is there increased, decreased, or normal arm swing?
- Turning: is there turning with difficulty, or en bloc turning?
- Step height: is the step height normal, reduced, or increased step height?
- Posture: is it upright or stooped?
- Stride length: is there normal stride length or reduced stride length?
- Is the patient:
- Able to do a tandem gait?
- Able to do heel walking?
- Able to toe walking?
- Is there any presence of a foot drop?
- Is there a positive or negative pull test (retropulsion)?
- With the patient standing, the examiner stands behind the patient (with a wall behind the examiner!), put hands on the patient’s shoulders, and say “At the count of three, I’m going to pull you back a little.”
- On a normal exam: the patient will take a step or two back or bend the shoulders backwards to keep maintain balance when pulled back.
- In a Parkinson's patient: the patient will either take many steps backwards (“retropulsion”), or fall over like a statue (“falling en bloc”).
- Is there astasia-abasia[11]
- Astasia is the inability to maintain an upright body position without assistance in the absence of motor weakness or sensory loss.
- Abasia is described as the inability to walk or as uncoordinated walking, while preserving mobility of the lower limbs.
Reflexes
- Reflexes are graded on a scale of 0 to 4:
- 0 = no reflexes
- 1 = decreased reflexes
- 2 = normal reflexes
- 3 = hyperreflexia
- 4 = hyperreflexia with clonus
- Upper extremity reflexes (biceps, brachioradialis, triceps)
- Lower extremity reflexes (patellar, Achilles)
- Babinski sign
No Knee Reflexes?
Try the Jendrassik maneuver and ask the patient to clench their teeth, flex both sets of fingers into a hook shape, and interlock those fingers together. The tendon below the patient's knee is then hit with a reflex hammer to elicit the patellar reflex.Tests of Reflex
| Exam | Pathological Response | |
|---|---|---|
| Upper extremity and lower extremity reflexes | Strike areas with tendon hammer to elicit reflex | Hyperreflexia is associated with upper motor neuron disease. Hyporeflexia is associated with lower motor neuron disease or with decreased sensation. |
| Babinski sign | Stroke along the sole (bottom) of the foot with a pointed end | A flexor plantar response is the normal response. The Babinski sign consists of dorsiflexion and fanning of the toes and indicates an upper motor neuron lesion |
Mnemonic
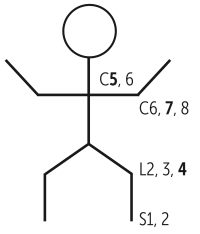
The mnemonic below can be used to remember the clinical reflexes (bold = main nerve root):
- Achilles reflex = S1, S2 (“buckle my shoe”)
- Patellar reflex = L2-L4 (“kick the door”)
- Biceps and brachioradialis reflexes = C5, C6 (“pick up sticks”)
- Triceps reflex = C6, C7, C8 (“lay them straight”)
- Cremasteric reflex = L1, L2 (“testicles move”)
- Anal wink reflex = S3, S4 (“winks galore”)
Sensory
- Are there normal sensation thresholds to all primary modalities (vibration, position, pin prick, temperature)?
- Romberg Test/Sign
- Instruct the patient to stand upright with their eyes closed for several seconds.
- The test is positive if the patient has significant swaying.
- The Romberg tests for disturbances in proprioception (not cerebellar function as often erroneously thought of) that indicates neuropathy, or posterior column disease.
Other Findings
- Agnosia is an individual's inability to correctly interpret signals from their five senses. Individuals with Alzheimer's disease may not recognize familiar people and objects. A common yet often unrecognized agnosia is the inability to appropriately perceive visceral, or internal, information such as a full bladder or chest pain.
- Teapot sign (give away weakness) - functional weakness
- Pinky sign - if someone is not giving full effort, when testing finger extension, the pinky will not go up
- The Hoover sign - functional weakness of lower extremity
- Closing eyes during reflexes can help to elicit true reflexes