- Last edited on May 30, 2020
Biopsychosocial Model and Case Formulation
Primer
The Biopsychosocial Model and Case Formulation (also known as the Biopsychosocial Formulation) in psychiatry is a way of understanding a patient as more than a diagnostic label. Hypotheses are generated about the origins and causes of a patient's symptoms. The most common and clinically practical way to formulate is through the biopsychosocial approach, first described in 1980 by George Engel.[1] Biopsychosocial formulation combines biological, psychological, and social factors to understand a patient, and use this to guide treatment and prognosis. Your formulation of a patient evolves and changes as you collect more information. There are other ways to formulate, including cognitive behavioural and psychodynamic approaches.

PsychDB is an Amazon Associate and earns from qualifying purchases. Thank you for supporting our site!
Diagnosis versus Formulation
Diagnosis is not the same as formulation! In mental health, when there is a group of consistent symptoms seen in a population, these symptoms can be categorized into a distinct entity, called a diagnosis (this is what the DSM-5 does). For example, we diagnose someone with a major depressive episode if they meet 5 of the 9 symptomatic criteria. However, formulation tells us how the person became depressed as a result of their genetics, personality, psychological factors, biological factors, social circumstances, and their environment.
You are probably already formulating, but just don't know it. Like most things in medicine, there are multifactorial causes of diseases, illnesses, and disorders. For example, type II diabetes does not develop because of a single pathophysiological cause. The patient may have a strong family history of the disease, a sedentary job, environmental exposures, and/or a nutritionally-poor diet. These factors all combine to cause the person to develop diabetes. Understanding how each factor contributes to a disease can better guide treatment decisions. In psychiatry, formulation appears more complicated because human behaviour and the brain itself is extraordinarily complex. However, like with anything, the more you practice, the better you will become at formulating.
What Are You Formulating?
You should always ask yourself: What exactly am I formulating? (i.e. - what are you trying to understand about the patient?) Usually it is their current symptoms or presentation (i.e. - the History of Presenting Illness, or HPI), but it is not always going to be the case. In some cases there may not be any current symptoms to formulate, and you may instead want to formulate the most recent episode of illness, the lifelong psychiatric diagnosis, or perhaps the patient's chronic thoughts of suicide (just to name a few examples).Why is a Biopsychosocial Approach Important?
This is why! The Parable of Panic: Suffocation, Social Attachment, and the Critical Role of an Integrative, Biopsychosocial FormulationThe 4 Ps
Formulation in a Nutshell
“Formulation asks what is wrong, how it got that way, and what can be done about it.”[2]The biopsychosocial model considers the “4 Ps” for each of biological, psychological, and social:
- Predisposing factors are areas of vulnerability that increase the risk for the presenting problem. Examples include genetic predisposition for depressive illness and prenatal exposure to alcohol.
- Precipitating factors are typically thought of as stressors or other events (they could be positive or negative) that may be precipitants of the symptoms. Examples include conflicts about identity or separation-individuation that arise at developmental transitions, such as puberty onset or graduation from high school.
- Perpetuating factors are any conditions in the patient, family, community, or larger systems that exacerbate rather than solve the problem. Examples include unaddressed relationship conflicts, lack of education, financial stress, and occupation stress (or lack of employment)
- Protective factors include the patient’s own areas of competency, skill, talents, interest and supportive elements. Protective factors counteract the predisposing, precipitating, and perpetuating factors.
The Table
Biopsychosocial Model
Adapted from Barker P. The child and adolescent psychiatry evaluation: basic child psychiatry. Oxford, UK: Blackwell Scientific, Inc. 1995.| Biological | Psychological | Social | |
|---|---|---|---|
| Predisposing (What is their “set up?” What were they working with initially?) | • What is their temperament? • What do we know about their consistent personality characteristics? • What is their family psychiatric history? • Are there toxic exposures in utero, birth complications, or developmental disorders? • Is there a history of concussions or traumatic brain injuries? | • What is their attachment style? • How did their family act? • Do they have problems with affect modulation? • Do they have a rigid or negative cognitive style? • Low self-image/self-esteem? | • Poverty, low socioeconomic status, teenage parenthood, poor access to health or mental health care. • Childhood exposure to maternal depression and domestic violence, late adoption, temperament mismatch, marital conflicts. |
| Precipitating (What acute event happened and how did it affect them?) | • Serious medical illness or injury? • Increasing use of alcohol or drugs? | • Conflicts around identity or separation-individuation arising at developmental transitions, such as puberty onset or graduation from high school? | • Loss of or separation from close family member, family move with loss of friendships, interpersonal trauma • Recent immigration, loss of home, loss of a supportive service (eg, respite services, appropriate school placement) |
| Perpetuating (What chronic things are going on?) | • Do they have a chronic illness, functional impairment caused by cognitive deficits, or a learning disorder? • Lack of medication optimization (suboptimal doses) • Lack of treatment or follow up for mental illness • Current substance use • Chronic medical issues and chronic pain • How is patient responding to hospitalization? • What are the degree of the symptoms right now? | • What are their beliefs about self/others/world? What ideas have they internalised? • Is there use of self-destructive coping mechanisms, help-rejecting personality style, or traumatic re-enactments? • Poor coping skills, limited or lack of insight • Personality traits (e.g. - unable to maintain consistent interpersonal relationships in borderline personality) • Potentially could discuss attachment style | • How do they seem to act in relationships over time? • Chronic marital discord, lack of empathy of parent, developmentally inappropriate expectations • Chronically dangerous or hostile neighbourhood, trans-generational problems of immigration, lack of culturally competent services • Chronic discord in relationships • Ongoing transitions • Poor finances • Working long hours • Isolation, unsafe environment |
| Protective (What is protecting them and keeping them well?) | • What is their overall health (healthy otherwise)? • What is their response to medications (good response/no response, did they achieve remission, are they optimized on current medications)? • Do they have above-average intelligence, easy temperament, resiliency, specific talents or abilities, or physical attractiveness? • No substance use is a protective factor | • Do they have ability to be reflective or modulate their affect? • Do they have a positive sense of self, or adaptive coping mechanisms? • Psychologically-minded • Good coping skills • Good insight | • Positive parent-child relationships, supportive community and extended family • Religious/spiritual beliefs • Community cohesiveness, availability of supportive social network, well-functioning child/family team • Good interpersonal supports • Financial support • Disability support • Has GP, psychiatrist, social, or case worker |
Filling out the Table
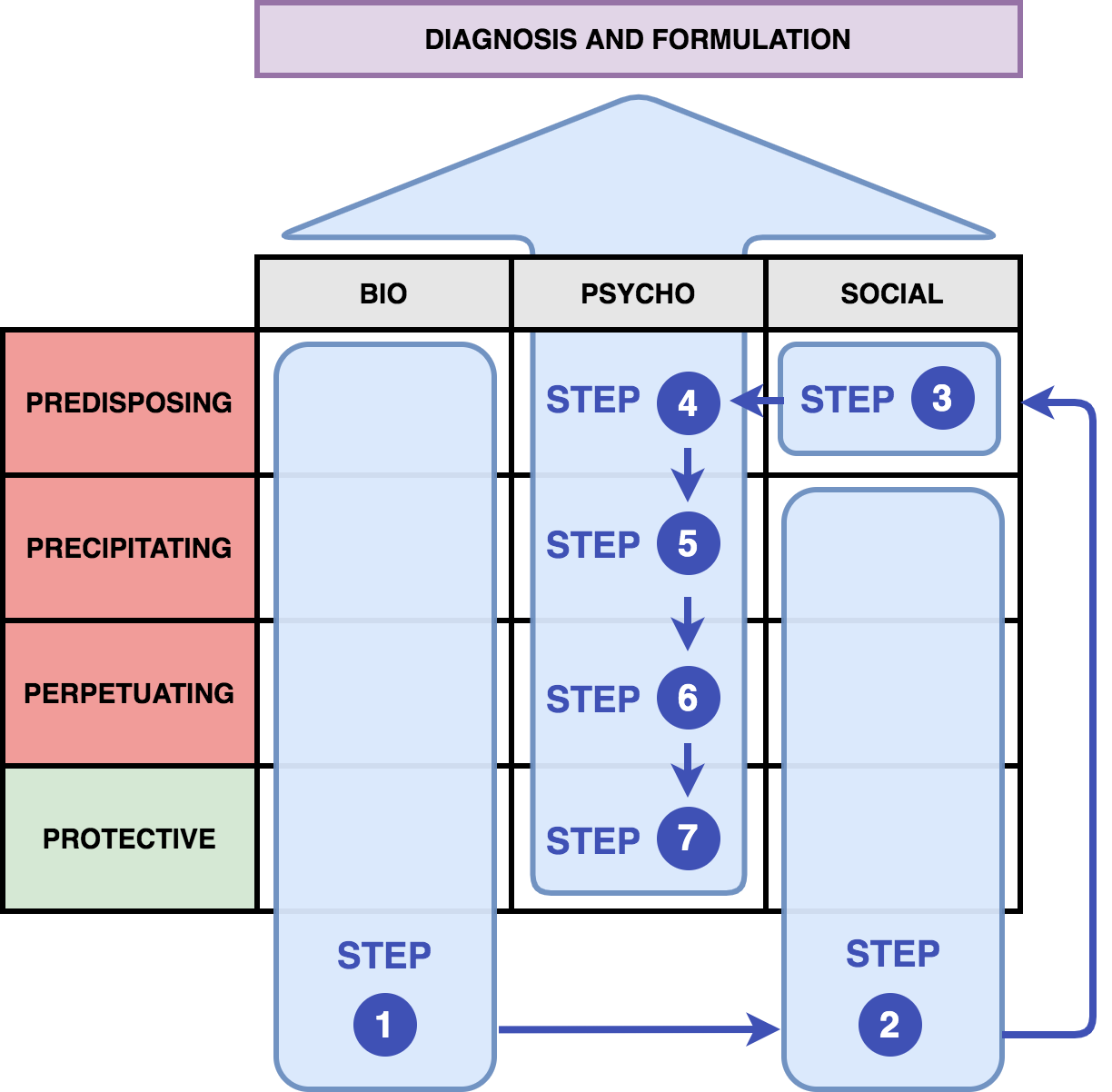
That's a lot of questions to ask and a lot of things to think about. Let's do a real life example, and fill out a biopsychosocial table using the guide on the right. The table below (figure 1) provides a guide to tell you where you should slot patient information and how to fill a formulation table. As a general rule, biological factors + social factors = (development of) psychological symptoms. These psychological symptoms are collected by the clinician to give a psychiatric diagnosis. This is why the psychological section of the table is filled last, so we can understand what biological and social factors led to the development of these symptoms.
Patient: Jane Doe
- Jane Doe is a 30-year-old female who presents to an emergency room with acute suicidal ideation.
- She has a past history of borderline personality disorder, depression, and alcohol use disorder (moderate). She used to be a soccer player and has a history of multiple concussions.
- Family history is significant for depression and bipolar. Social history is significant for parental divorce at age 5, and multiple unstable relationships lasting only weeks to months at a time. Experienced sexual abuse at age 12.
- Developmentally, there may have been some developmental speech delay.
The "Three Squares" Model
Most of the table can be easily filled in from the history gathered in your psychiatric interview. The hardest part is what we'll call the “3 squares”: predisposing social factors (Step 4), predisposing psychological factors (Step 5), and precipitating psychological factors (Step 6). This is where you'll need to be creative and also think more in-depth about your patient. This is usually the hardest part of the patient to formulate.
Jane Doe
| Step 4 | Social (Predisposing) | Early parental divorce, unstable home life |
|---|---|---|
| Step 5 | Psychological (Predisposing) | (Led to) fears of abandonment then developed early in childhood |
| Step 6 | Psychological (Precipitating) | Re-experienced these feelings of abandonment after breakup with boyfriend |
Another Example
| Step 4 | Social (Predisposing) | Absent father, abusive mother, unstable home life |
|---|---|---|
| Step 5 | Psychological (Predisposing) | Long-standing feelings of isolation and insecurity since childhood |
| Step 6 | Psychological (Precipitating) | Joined a gang, entering a stressful lifestyle, led to increased hyper-vigilance and paranoia in the past few months |

Sample Table
Sample Formulation #1
| Biological | Psychological | Social | |
|---|---|---|---|
| Predisposing |
|
|
|
| Precipitating |
|
|
|
| Perpetuating |
|
|
|
| Protective |
|
|
|
Presenting your Formulation
There is no “right” or “wrong” way to present a formulation. The most important thing about formulation is that it should be intuitive and flow logically. The biopsychosocial table and examples above provides one example of a very structured formulation, but here are 3 other presentation styles you can also consider.
Method 1
Here are the key points that should be addressed when presenting your formulation:
- Brief summarizing statement that includes demographic information, chief complaint, and presenting problems from patient's perspective and course (onset, severity, pattern) of signs and symptoms
- Precipitating stressors or events
- Biologic factors
- Psychological factors
- Sociocultural, family, interpersonal, and environmental factors
- Strengths and protective factors of the patient
- Role performance, including level of functioning in major areas of daily life
- Integrative statement: how the factors interact to lead to the current situation and level of functioning, prognosis, and potential openings for intervention
- Problem list
- Treatment plan
Method 2
Another way of presenting a formulation of a patient could be as follows:
- Furthermore, these problems can be understood as arising from the following developmental processes:
- Childhood/adult trauma (if any)
- Attachment style
- … which has led to the following thinking patterns:
- About themselves
- About others
- About the world
- … and the [precipitating event] (i.e. - current stressor) is connected to their underlying struggles in the following way:
- e.g. - Their depression was brought on by the (i) death of their spouse, (ii) stopping medications, (iii) loss of job, (iv) experiencing of trauma, etc.
- They have the following protective factors:
- Biological: No substance use
- Psychological: Resilience
- Social: Strong support from family, psychiatrist, social worker, children, pets, family
Method 3
Another way to present a formulation is in chronological order, starting from birth:
- Genetics (family history)
- Birth (issues at birth)
- Childhood (attachment style, neurodevelopment, milestones, trauma)
- Adolescence (relationships, trauma, school performance, substances)
- Adulthood (occupation, relationships, children, environment, stressors)
Common Phrases to Use
- Psychological Predisposing Factors
- “Used substances as a coping style in adolescence/young adult, and now this is playing out again in adulthood due to this vulnerability.”