Table of Contents
Biopsychosocial Model and Case Formulation
Primer
The Biopsychosocial Model and Case Formulation (also known as the Biopsychosocial Formulation) in psychiatry is a way of understanding a patient as more than a diagnostic label. Hypotheses are generated about the origins and causes of a patient's symptoms. The most common and clinically practical way to formulate is through the biopsychosocial approach, first described in 1980 by George Engel.[1][2] Biopsychosocial formulation combines biological, psychological, and social factors to understand a patient, and uses this to guide both treatment and prognosis. Your formulation of a patient evolves and changes as you collect more information. Formulation is like cooking, and there is no 'right' or 'wrong' way to do it, but most get better over time with increasing clinical experience.
PsychDB is an Amazon Associate and earns from qualifying purchases. Thank you for supporting our site!
Diagnosis versus Formulation
Diagnosis is not the same as formulation! In mental health, when there is a group of consistent symptoms seen in a population, these symptoms can be categorized into a distinct entity, called a diagnosis (this is what the DSM-5 does). For example, we diagnose someone with a major depressive episode if they meet 5 of the 9 symptomatic criteria. However, formulation tells us how the person became depressed as a result of their genetics, personality, psychological factors, biological factors, social circumstances (childhood adverse events and social determinants of health), and their environment.
You are probably already formulating, but just don't know it. Like most things in medicine, there are multifactorial causes of diseases, illnesses, and disorders. For example, type II diabetes does not develop because of a single pathophysiological cause. The patient may have a strong family history of the disease, a sedentary job, environmental exposures, and/or a nutritionally-poor diet. These factors all combine to cause the person to develop diabetes. Understanding how each factor contributes to a disease can better guide treatment decisions. In psychiatry, formulation appears more complicated because human behaviour and the brain itself is extraordinarily complex. However, like with anything, the more you practice, the better you will become at formulating.
What Are You Formulating?
Each time you formulate, always ask yourself: What exactly am I formulating? (i.e. - what are you trying to understand about the patient?) Usually it is their current symptoms or presentation (i.e. - the History of Presenting Illness, or HPI), but it is not always going to be the case. In some cases there may not be any current symptoms to formulate, and you may instead want to formulate the most recent episode of illness, the lifelong psychiatric diagnosis, or perhaps the patient's chronic thoughts of suicide (just to name a few examples).Why is a Biopsychosocial Approach Important?
This is why! The Parable of Panic: Suffocation, Social Attachment, and the Critical Role of an Integrative, Biopsychosocial FormulationThe 4 Ps
Formulation in a Nutshell
“Formulation asks what is wrong, how it got that way, and what can be done about it.”[3]The biopsychosocial model considers the “4 Ps” for each of the biological, psychological, and social factors:
- Predisposing factors are areas of vulnerability that increase the risk for the presenting problem. Examples include genetic (i.e. -family history) predisposition for mental illness or prenatal exposure to alcohol.
- Precipitating factors are typically thought of as stressors or other events (they could be positive or negative) that may be precipitants of the symptoms. Examples include conflicts about identity, relationship conflicts, or transitions.
- Perpetuating factors are any conditions in the patient, family, community, or larger systems that exacerbate rather than solve the problem. Examples include unaddressed relationship conflicts, lack of education, financial stresses, and occupation stress (or lack of employment)
- Protective factors include the patient’s own areas of competency, skill, talents, interest and supportive elements. Protective factors counteract the predisposing, precipitating, and perpetuating factors.
The Formulation Table
The “4 Ps” can be laid out in a 3 x 4 table to systematically do formulation and identity factors. Note that this table is extremely comprehensive and long, and not everything will (or should!) apply to your case. It is important to remember that not everything will fit neatly into each box. For example, many precipitating and perpetuating factors may overlap and fit in other boxes. Use this table as a general guide, but don't memorize it for the sake of memorizing it!
Biopsychosocial Model
Adapted from Barker P. The child and adolescent psychiatry evaluation: basic child psychiatry. Oxford, UK: Blackwell Scientific, Inc. 1995, and from Weerasekera, P. (1993). Formulation: A multiperspective model. The Canadian Journal of Psychiatry.| Biological | Psychological | Social | |
|---|---|---|---|
| Predisposing (What is their “set up?” What were they working with initially?) | • What was their temperament at birth? • What do we know about their consistent personality characteristics? • Is there a family psychiatric history? • Are there toxic exposures in utero, birth complications, or developmental disorders? • Is there a history of concussions or traumatic brain injuries? • Neurodevelopmental history | • What is their attachment style? • How did their family act and what is the family structure (i.e. - did the patient model their parent's behaviours, or did they rebel against their parent's behaviours – you either “act like your parents” or “act the opposite of your parents because you don't want to be like them”)? • Do they have problems with affect modulation? • Do they have a rigid or negative cognitive style? • Low self-image/self-esteem? | • Poverty, low socioeconomic status, teenage parenthood, or poor access to health care? • Childhood exposure to maternal depression, domestic violence, late adoption, temperament mismatch, or marital conflicts? • Immigration history, marginalization, discrimination, or racism? • Exposure to antisocial personality/traits |
| Precipitating (What acute event happened and how did it affect them?) | • Serious medical illness or injury? • Increasing use of alcohol or drugs? • Medication non-adherence? • Pregnancy or hormonal changes? • Sleep deprivation? | Stressor that activate one or more psychological processes: • Cognitive: core beliefs and cognitive distortions • Dialectical: emotional dysregulation and dysfunction • Interpersonal: grief, loss, disagreement, change/transitions • Psychodynamic: unconscious conflicts/defenses, and unconscious repetition of early relationship patterns (psychic determinism) | • Loss of or separation from close family, partner, or friends • Interpersonal trauma • Work/academic/financial stressors • Recent immigration, loss of home, loss of a supportive service (e.g. - respite services, appropriate school placement) • Is the individual's current experience/symptoms similar to a past situation (i.e. - “history repeating itself”)? For example, they might have had a loss, separation etc. in the past |
| Perpetuating (What chronic things are going on?) | • Do they have a chronic illness, functional impairment caused by cognitive deficits, or a learning disorder? • Lack of medication optimization (suboptimal doses) • Lack of treatment or follow up for mental illness • Current substance use? • Chronic medical problems, chronic pain, or disability? • How is patient responding to hospitalization? • What are the degree of the symptoms right now? | One or more perpetuating psychological processes: • Cognitive: chronic negative thoughts and reinforcing environment • Dialectical: help-seeking and help-rejecting, chronic emotional dysregulation and poor distress tolerance • Interpersonal: Chronic/unresolved dysfunctional relationships, interpersonal conflicts, or role transitions • Psychodynamic: recurring themes throughout one’s life, chronic primitive defenses • What are their beliefs about self/others/world? What ideas have they internalized? • Are there self-destructive coping mechanisms, or traumatic re-enactments? • Ongoing poor coping skills, limited or lack of insight? • Personality traits (e.g. - unable to maintain consistent interpersonal relationships in borderline personality disorder) • How is their attachment style playing out in this particular situation? | • Chronic marital/relationship discord, lack of empathy from family/friends, developmentally inappropriate expectations • Chronically dangerous or hostile neighbourhood, trans-generational problems of immigration, lack of culturally competent services • Ongoing transitions and stressors • Poor finances or working long hours • Isolation, unsafe environment |
| Protective (What is protecting them and keeping them well?) | • Good overall health • Absence of family psychiatric history • What is their response to medications (good response/no response, did they achieve remission, are they optimized on current medications)? • Do they have above-average intelligence, easy temperament, resiliency, specific talents or abilities? • No substance use is a protective factor | • Do they have ability to be reflective or modulate their affect? • Do they have ability to mentalize (see other's perspectives)? • Do they have a positive sense of self, or adaptive coping mechanisms? • Psychologically-minded, reflective, and capacity to change thinking patterns? • Have they previously responded well to therapy? • Good coping skills, good insight? | • Positive relationships, supportive community, and/or extended family/friends? • Religious/spiritual beliefs • Good interpersonal supports • Financial/disability support • Has an outpatient healthcare team: GP, psychiatrist, social, or case worker? |
Filling out the Table
- As you can see in the table above, it's a lot of questions to ask and a lot of things to think about!
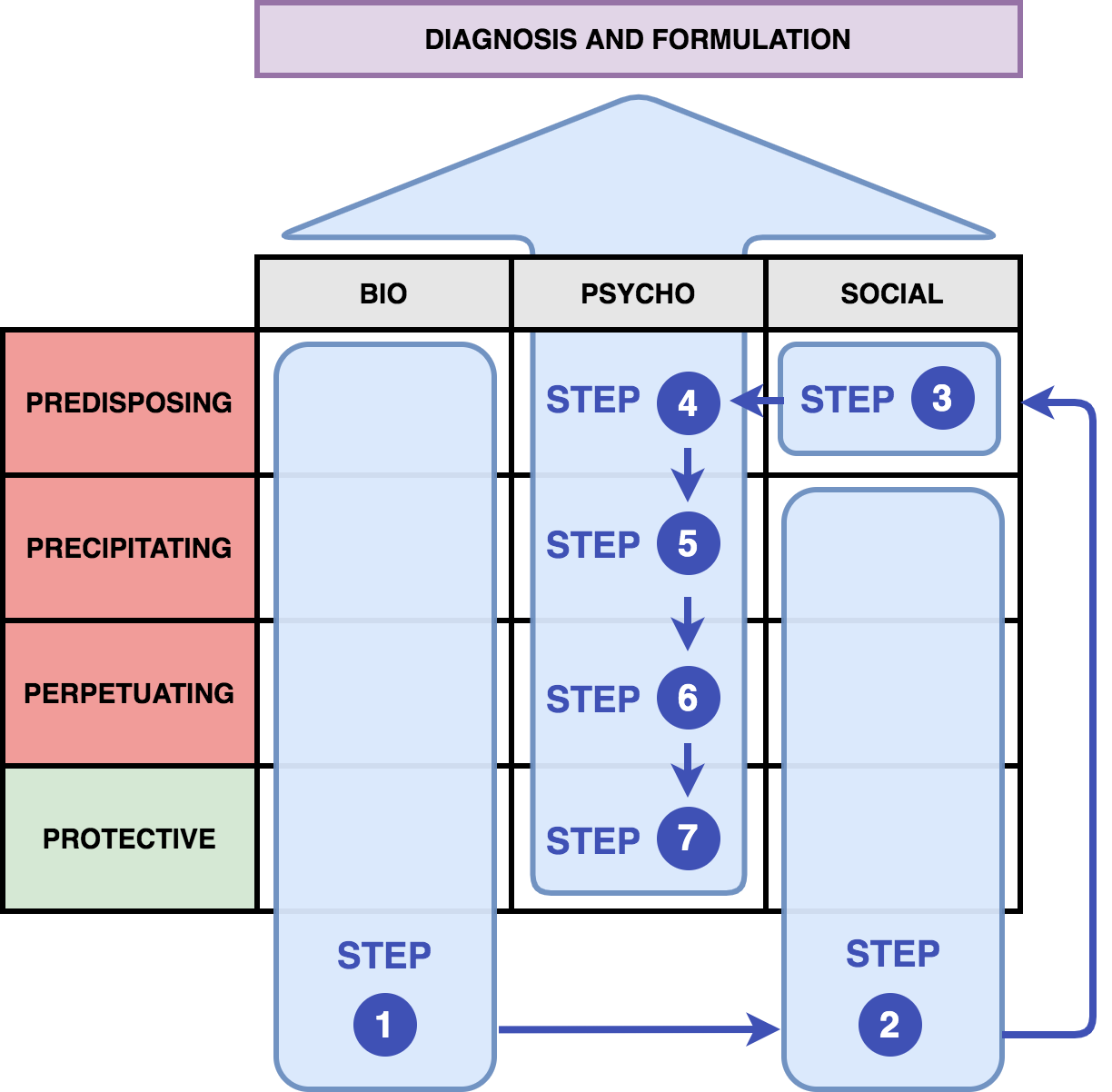
- Let's do a simplified formulation for the patient (Jane Doe) below. The image (figure 1) provides a guide on how to put information into the formulation table.
- As a general rule, when you are filling out the table, try to remember that biological factors + social factors → (lead to development of) psychological symptoms/factors.
- These psychological symptoms/factors are then observed by the clinician to give a psychiatric diagnosis.
- This is why the psychological section of the table is filled last, so we can understand what biological and social factors led to the development of these symptoms.
"Jane Doe"
- Patient ID:
- Jane Doe is a 30-year-old female who presents to the emergency room with acute suicidal ideation and self-harm
- History of Presenting Illness:
- Jane has been working at a start up company for the past 2 years. She was suddenly fired from her job today due to conflicts at work with co-workers and being late at work several times from sleeping in. After being told she was fired from her job, she went home and self-harmed to cope with the distress of this loss. She also drank 10 beers prior to arriving in the hospital. She subsequently planned to overdose on her medications. A concerned best friend called and talked to her this evening, and brought her to the hospital. Her mood was stable prior to this job loss, and she had no self-harm or suicidal thoughts in the past 1 year.
- Substance Use History:
- Increasing alcohol use for the past 3 months, drinking up to 5 beers per day.
- Medication History:
- Sertraline (Zoloft) 75mg PO daily
- Past Medical and Psychiatric History:
- She has a past history of borderline personality disorder, depression, and alcohol use disorder (moderate). She used to be a soccer player and has a history of multiple concussions. She does have a psychiatrist that she sees every month. She previously completed a course of dialectical behavioural therapy, which was helpful.
- Family History:
- Depression and bipolar disorder on maternal side of her family. There is a history of alcohol use disorder on paternal side.
- Social History:
- Born in Canada. University-educated. There was a parental divorce at age 5. She describes an invalidating childhood, where parents did not acknowledge or praise her. She experienced sexual abuse and trauma at age 12. She is in a 2-year relationship with a male partner, and there have been recent arguments about the direction of their relationship. She describes a long-standing fear of being abandoned in relationships, and reports having very intense relationships with friends/family. Financially, she is struggling to pay rent and living from paycheque-to-paycheque. Developmentally, there may have been some speech delay. Collateral information from the patient's older brother describe her childhood temperament as being avoidant and fearful of her parents.
Biological and Social Factors
Steps 1 and 2
OK, we can start by filling out the “easy” stuff first for Jane Doe. We can go down the table and start identifying biological factors (Step 1), followed by most of the social factors (Step 2) based on the history we have above. We'll leave the predisposing social factor and psychological factors for the end.Sample Formulation for Jane Doe
| Biological | Psychological | Social | |
|---|---|---|---|
| Predisposing | • Family history of mental disorders and substance use • History of concussions • Fearful/anxious temperament at birth | Step 4 | Step 3 |
| Precipitating | • Increase in alcohol use in the last 3 months | Step 5 | • Recently fired from job |
| Perpetuating | • Current dose of sertraline is subtherapeutic • Ongoing alcohol use | Step 6 | • Ongoing discord in her romantic relationship • Ongoing financial difficulties |
| Protective | • Medically healthy | Step 7 | • Good interpersonal support from her best friend who brought her to hospital • Has a psychiatrist that she sees every month |
Psychological Factors
Now that you've filled in the easy parts from the history, the hardest part is conceptualizing the predisposing social factors (Step 3), and all of the psychological factors (Steps 4, 5, 6, 7). This is where you'll need to be creative and also think more in-depth about your patient. Ideally, each step should flow logically and intuitively into the next based on your framework, as you'll see in our case of Jane Doe. Having a framework for understanding of different psychological treatments and psychological theories can be helpful in making your psychological formulation flow intuitively (e.g. - attachment theory, cognitive behavioural therapy, dialectical behavioural therapy, interpersonal therapy, psychodynamic therapy). However, this can be done intuitively even without an in-depth understanding of these frameworks (we don't need to be Freud to do this). The more cases you go through (and more of the sample formulations below) the more comfortable you will be with formulating!
Steps 3, 4, 5, 6, and 7
Let's give it a try now and understand the patient's psychological factors through a developmental/trauma and dialectical behavioural therapy framework. Note that we could also formulate her through other frameworks, but this one is the most intuitive for her history and current presentation.Jane Doe's Formulation
| Step | Factor | Description |
|---|---|---|
| Step 3 | Social (Predisposing) | Early parental divorce, unstable home life, history of trauma. History of invalidation and lack of acknowledgement by parents |
| Step 4 | Psychological (Predisposing) | (Led to) fears of abandonment which developed early in childhood |
| Step 5 | Psychological (Precipitating) | Re-experienced these feelings of abandonment after being fired from work |
| Step 6 | Psychological (Perpetuating) | Lack of adaptive coping mechanisms resulted in using self-harm to cope and avoid further emotional dysregulation. Additionally, the lack of coping mechanisms leading to intense thoughts of suicide. |
| Step 7 | Psychological (Protective) | Previously responded well to DBT, and has a history of being psychologically-minded and insightful. University educated. |
Completed Table
Completed Biopsychosocial Formulation Table
Hooray! Now we have that filled out the rest of the table, let's put it all together.Completed Formulation of Jane Doe
| Biological | Psychological | Social | |
|---|---|---|---|
| Predisposing | • Family history of mental disorders and substance use • History of concussions • Fearful/anxious temperament at birth | • Fears of abandonment which developed early in childhood • History of invalidation and lack of acknowledgement by parents | • Early parental divorce, unstable home life, history of trauma |
| Precipitating | • Increase in alcohol use in the last 3 months | • Re-experienced these feelings of invalidation and abandonment after being fired from work | • Recently fired from job |
| Perpetuating | • Current dose of sertraline is subtherapeutic • Ongoing alcohol use | • Her lack of adaptive coping mechanisms resulted in using self-harm to cope • Additionally, the lack of coping mechanisms leading to intense thoughts of suicide | • Ongoing discord in her romantic relationship • Ongoing financial difficulties |
| Protective | • Medically healthy | • Previously responded well to DBT • History of being psychologically-minded and insightful • University educated | • Good interpersonal support from her best friend who brought her to hospital. • Has a psychiatrist that she sees every month |
Presenting your Formulation
You've got your table all filled out now. Now what? How do you present all this information and data? Remember there is no “right” or “wrong” way to present your formulation. But the most important thing about formulation is that it should be intuitive and flow logically. Some different presentation styles are suggested here.
Method 1 (Sequential)
The “4 Ps” formulation table can be a very rigid and systematized way of presenting a formulation. At its most basic, you could present each box sequentially and describe each factor. Most learners will use this method as it is the most “simple.” It is usually presented as Predisposing → Precipitating → Perpetuating → Protective factors. As you get better and more expert at formulating, you may not need to use this rigid structured format, and instead, will be able to present a more intuitive and organic formulation of the patient instead (see other methods below).
- Brief summarizing statement that includes demographic information, chief complaint, and presenting problems from patient's perspective and signs and symptoms (onset, severity, pattern)
- Predisposing factors
- Precipitating factors
- Perpetuating factors
- Strengths and protective factors
- Integrative statement: how these factors interact to lead to the current situation and level of functioning, prognosis, and potential openings for intervention
Example: 4 Ps Table Formulation of Jane Doe
- Jane Doe presents with a diagnosis of borderline personality disorder and history of depression. She presents to hospital today with acute suicidal ideation and self-harm after being fired from her job.
- Predisposing factors: Her predisposing biological factors include a family history of mental disorders and substance use, concussion history, and a fearful/anxious temperament at birth. Her predisposing social factors include a history of sexual trauma at a young age, and early parental divorce. These led to her predisposing psychological factors, including a history of invalidation by her parents, and fears of abandonment during childhood.
- Precipitating factors: Her precipitating biological factors include a 3-month history of increasing alcohol use. Her precipitating social factors is her being fired from her current job. These led to her precipitating psychological factors, which resulted in her underlying feelings of abandonment and invalidation re-activated after being fired from work.
- Perpetuating factors: Her perpetuating biological factors include being on a subtherapeutic dose of her medication, and her ongoing alcohol use. Her perpetuating social factors includes her ongoing relationship conflicts and financial stressors. Her perpetuating psychological factors include her lack of adaptive coping strategies and ongoing self-harm.
- Strengths and protective factors: She is medically healthy, and has previously responded well to therapy. She also is supported by a good friend, and sees a psychiatrist regularly.
- Integrative Statement: The acute stressor of losing her job has re-activated the psychological processes described above. The patient is psychologically minded and thus would benefit from treatment with dialectical behavioural therapy. Her medications could also be further optimized as well. Overall, her prognosis is good due to her protective factors as mentioned above.
Method 2 (Narrative)
The narrative formulation of the patient is a less rigid presentation structure where you may not choose to present everything in the 4 Ps table, and instead focus on the key factors that you think are relevant:
- [Patient] presents with a [diagnosis]. They are biologically predisposed because of [reasons]. They struggle with the following [psychological difficulties]. Their underlying temperament is [temperament], which further exacerbates the symptoms.
- Furthermore, the patient's difficulties can be understood as arising from the following developmental processes:
- Childhood/adult trauma (if any)
- … which has led to the following thinking patterns:
- About themselves
- About others
- About the world
- … and the [precipitating event] is connected to their underlying struggles in the following way:
- e.g. - depression was brought on by the:
- (i) death of their spouse
- (ii) stopping medications
- (iii) loss of job
- (iv) re-experiencing of trauma
- They have the following: [protective factors]
Example: Narrative Formulation of Jane Doe
- Jane Doe presents with a diagnosis of borderline personality disorder and history of depression. She is biologically predisposed, with a family history of depression and alcohol use disorder in her immediate family members. She struggles with the following psychological difficulties, including fears of abandonment. Her underlying temperament is anxious, which further exacerbates her symptoms.
- Furthermore, the patient's difficulties can be understood as arising from the following developmental processes:
- Her underlying history of experiencing trauma and sexual abuse at a young age
- A history of invalidating experiences in childhood
- … which has led to the following thinking patterns:
- That she is not deserving of love or close relationships, a core belief of her being “unlovable”, and that self-harm is the main way of coping with stressors
- That others may leave or abandon her any time, increased rejection sensitivity, and a future fear of being rejected
- That the world can be a fearful and scary place
- … and her being fired from her job is connected to her underlying struggles in the following way:
- After being fired from her job, she experienced strong feelings of rejection, and was unable to cope with this major stressor. This may have reactivated/exacerbated her emotional dysregulation, and resulted in negative coping styles such as her self-harming and suicidal ideation. She also appears to use alcohol as a way of managing distressing emotions, but does not have any psychological coping strategies. This has further exacerbated her alcohol use disorder.
- She has the following protective factors, including a supportive psychiatrist and friend. She has also previously responded well to psychotherapy and appears to be psychologically-minded.
Method 3 (Advanced)
A much more advanced and nuanced presentation might be using a more comprehensive formulation that integrates the 4Ps formulation through multiple lenses (e.g. - Eriksonian developmental stages, psychodynamic defenses, and dialectical behavioural):
- Patient ID
- Current stressors, plus salient developmental history
- “The patient presents at this time with [problem and symptoms], in the context of [situation and stressors]”
- Non-psychological factors:
- Genetics, temperament, medical history, substances, medications
- “The patient has the following [genetic vulnerabilities, medical history]”
- Early developmental and pathogenic psychological factors:
- Pathogenic psychological factors
- “The patient grew up in a family characterized by [factors], with a caregiver who was [distant/available/invalidating]”
- Capacity for interaction, communication, empathy, and attachment
- “Attachment was likely [secure/insecure/disorganized] given [developmental history]”
-
- “The patient may have had difficulty in [stage of development], and this is reflected in [examples from adult relationships]
-
- “It appears that the patient may have struggled with conflicts in early life. It also appears they may have had difficulty with [drives], stemming from [psychoanalytic concept]
- Control/regulation of drives
- Self-perception and self-image
- “These experiences impacted the patient's view of themselves as being [view of self], and this has continued into adulthood based on [experiences].”
- Defense mechanisms and coping
- “The patient appears to have adopted [defense mechanisms] as coping strategies by early adulthood, and these have continued on…”
- Characteristic patterns of interpersonal relationships
- “The patient's interpersonal relationships appear to be [give examples of patterns of relationships]”
- Precipitating and perpetuating factors
- These underlying factors may have precipitated the patient's [current presentation]. These symptoms have been maintained by [psychological factors/personality factors], and [social/environmental factors]
- Prediction of response to treatment and interventions
- “We would anticipate when engaging in treatment, the patient may have [resistance/transference/countertransference]. However, patient has the following [protective factors], which may be a good prognostic factor. Based on these factors, the following [treatment and management] would be the most helpful for this patient.
Example: Advanced Formulation of Jane Doe
- Jane Doe is a 30-year-old female who presents with acute suicidal ideation in the context of a job loss. She notably has a past history of childhood trauma and abuse.
- The patient has genetic vulnerabilities for mental illness in her family history, a history of anxious temperament, ongoing substance use, and subtherapeutic medication levels.
- She has several early developmental and pathogenic psychological factors, including growing up in a family characterized by invalidation, with parents who were distant and unavailable. This likely led to an attachment style that was likely insecure and disorganized. Due to her history of abuse at age 12, she may have struggled with identity versus role confusion during that Eriksonian stage of psychosocial development. As she was unable to develop a sense of self and personal identity, these psychological factors are reflected in her adulthood with unstable relationships, and fears of abandonment. This has led to her adulthood self-perception of being unworthy of being loved, a constant fear of rejection, and increased rejection sensitivity. The patient appears to have adopted self-harming as a primitive coping strategy by early adulthood, and these have continued on in adulthood.
- Precipitating and perpetuating factors: the stressor of losing her job has reactivated these more primitive defense mechanisms and coping strategies. These symptoms have been further perpetuated by the personality factors and traits described above, and her ongoing financial stressors. Her ongoing alcohol use is another example of a maladaptive coping strategy.
- We would anticipate when engaging in treatment, the patient may have difficulties with using primitive defense mechanisms. However, the patient has protective factors including psychological mindedness and previous response to therapy, which is a good prognostic factor. Based on these factors, dialectical behavioural therapy would be the most helpful for this patient.
Method 4 (Chronological)
Yet another way to present a formulation is in chronological order, starting from birth until present time:
- Genetics (family history)
- Birth (issues at birth, developmental history, developmental stages)
- Childhood (attachment style, neurodevelopment, milestones, trauma)
- Adolescence (relationships, trauma, school performance, substances)
- Adulthood (occupation, relationships, children, environment, stressors)
- Integrative statement (of how genetics, birth, childhood, adolescence, and adulthood factors contribute to current presentation, and how this directs your treatment/management)
Common Phrases to Use
Having certain common phrases to use can be helpful to structure your presentation. Here are some examples:
- Biological Factors
- “From a biological perspective, the patient is vulnerable because…”
- Social Factors
- “The patient's early childhood and developmental history suggest…”
- “Used substances as a coping style in [the past], and now this is occurring again (or there is a relapse) due to [social factor].”
- Psychological Factors
- “Used substances as a coping style in [the past], and now this is occurring again (or there is a relapse) due to [psychological vulnerability].”
- “I wonder if… [psychological factor] is contributing to [current symptoms/struggles]”
Do's and Dont's
Do
- Use your own words and personal style
- Tell a story and narrative that is unique to your patient
- Be specific and demonstrate your understanding of the patient as a person and not a diagnosis
- Use words like precipitating, protective, and perpetuating factors to anchor your listener
- Focus on the most salient features and be concise
- Try and use a psychological theory (but only if you understand it)
- Be confident in your presentation!
Don't
- Include too much extra detail
- Try to be perfect only to overwhelm yourself
- Be generic (your formulation needs to be unique to your patient)
- Tell the patient's whole story all over again
- Mention life events or trauma without an understanding of its meaning or impact
- Try to formulate a “grand unified theory” of the patient and over-reach with your theory (if it doesn’t fit, it doesn’t fit! And that's okay!)
- Cover every box in the 4 Ps just for the sake of doing it (not all boxes will always apply!)
Beyond Basic Formulation
A good formulation should be integrative, and let you understand how all of the patient's factors interact to lead to the current situation. This gives you a sense of their current level of functioning, prognosis, and guides your direction for treatment and management decisions.
Treatment
A good biopsychosocial formulation allows you to come up with a comprehensive and holistic treatment plan for your patient. Here is an example of a set of treatment recommendations for Jane Doe:
- Disposition
- What level of care is required (outpatient or inpatient)?
- Jane is able to articulate a safe plan to stay with a friend, and is suitable for outpatient care
-
- Jane might benefit from an increase of her sertraline from 75mg to 100mg and beyond (maximum dose of 200mg), for her mood dysregulation and depressive symptoms
- Jane might benefit from the use of anti-craving medications such as gabapentin or acamprosate to reduce her cravings for alcohol use
-
- Dialectical behavioural therapy (DBT) would be the most appropriate for Jane
- Jane would also benefit from motivational interviewing for her alcohol use
- Long-term, Jane might also benefit from a more in-depth understanding of how her past trauma affects her present self and symptoms. This could be achieved with more specific and in depth trauma therapy, but given the acuity of her symptoms, this is something that would follow after DBT.
- Social
- Jane could benefit from accessing support from her company's HR department to understand what options she has after her job termination
- Substance use groups such as Alcoholic's Anonymous
- Increasing connections to her friends and social supports
Another Example
For good measure, here is another sample formulation for someone with a diagnosis of schizophrenia. Note that in this example, since the precipitating cause for acute psychosis (also applies to manic episodes) is more “biological,” it may be harder to identify underlying psychological factors (but that's OK too – even the most “biological” psychiatric disorders can often be precipitated by psychosocial stressors). Again let's fill out the easiest parts of the table first:
Sample Formulation for Schizophrenia (Initial)
| Biological | Psychological | Social | |
|---|---|---|---|
| Predisposing | • Family history of psychosis and schizophrenia | ? (Step 4) | ? (Step 3) |
| Precipitating | • History of cannabis use at early age | ? (Step 5) | • Social isolation and withdrawn from family members |
| Perpetuating | • Discontinuation of antipsychotics • Ongoing cannabis use and smoking, reducing the effectiveness of medications, and also exacerbating risk of psychosis | ? (Step 6) | • Ongoing social isolation due to psychosis causing him to be fearful of others |
| Protective | • Medically healthy • Previously responded to antipsychotic medications • No history of developmental delay or head injuries | ? (Step 7) | • Followed by an early intervention in psychosis team • Supported by girlfriend and several close friends • University educated |
Now here is one potential example of a predisposing social and psychological formulation of psychosis (again, there are no right or wrong ways to formulate, it depends on the patient you have in front of you!)
Example of A Possible Psychological Formulation of Psychosis/Schizophrenia
| Step | Factor | Description |
|---|---|---|
| Step 3 | Social (Predisposing) | • History of immigration (increases risk for psychosis) • Absent father, abusive mother, unstable home life |
| Step 4 | Psychological (Predisposing) | Long-standing feelings of isolation and insecurity since childhood |
| Step 5 | Psychological (Precipitating) | Joined a gang, entering a stressful lifestyle, led to increased hyper-vigilance and paranoia in the past few months |
| Step 6 | Psychological (Perpetuating) | • Ongoing delusions leading patient become suspicious of healthcare workers/family • Psychosis leading to poor insight, and inability to reality test. He is unable to understand that persecutory delusions are a function of his psychosis. |
| Step 7 | Psychological (Protective) | • Previously responded well to CBT for psychosis • Psychologically-minded and insightful when well |
Here's what the completed table would look like with the psychological factors incorporated.
Completed Formulation for Schizophrenia (Initial)
| Biological | Psychological | Social | |
|---|---|---|---|
| Predisposing | • Family history of psychosis and schizophrenia | Long-standing feelings of isolation and insecurity since childhood | • History of immigration (increases risk for psychosis) • Absent father, abusive mother, unstable home life |
| Precipitating | • History of cannabis use at early age | Joined a gang, entering a stressful lifestyle, led to increased hyper-vigilance and paranoia in the past few months | • Social isolation and withdrawn from family members |
| Perpetuating | • Discontinuation of antipsychotics • Ongoing cannabis use and smoking, reducing the effectiveness of medications, and also exacerbating risk of psychosis | • Ongoing delusions leading patient become suspicious of healthcare workers/family • Psychosis leading to poor insight, and inability to reality test. He is unable to understand that persecutory delusions are function of his psychosis. | • Ongoing social isolation due to psychosis causing him to be fearful of others |
| Protective | • Medically healthy • Previously responded to antipsychotic medications • No history of developmental delay or head injuries | • Previously responded well to CBT for psychosis • Psychologically-minded and insightful when well | • Followed by an early intervention in psychosis team • Supported by girlfriend and several close friends • University educated |
"Templates"
As you do more formulation, you will notice that patients tend to present in “templates,” that is, certain diagnoses tend to follow a certain common theme of predisposing, precipitating, and perpetuating factors. The more you formulate, it can be helpful to have a rough template of different formulations for different diagnoses (e.g. - depression, self-harm, mania/psychosis, anxiety, etc.) It will make your job of formulating much easier.
Resources
Readings
The following readings below are excellent resources to further develop your formulation skills: